
Building the Bonds of Attachment Review: Understanding Attachment and Healing

Photo by Vitaly Gariev on Unsplash
The Labyrinth of the Mind:
A Clinical and Empathic Guide to OCD
Erik Turley, LMFT
04/08/2026
If you find yourself trapped in a cycle of scary thoughts and tiring rituals, the first thing you need to know is that you are not broken. Obsessive-Compulsive Disorder (OCD) is a difficult brain-based challenge, but it is one that responds very well to the right treatment. By understanding the science behind the disorder and the specific ways it affects your life and family, you can begin the journey toward feeling better and winning back your freedom.
Defining the Cycle: Beyond the Myths of Neatness
People often joke about being “a little OCD” when they like a clean desk, but for the millions living with it, OCD is a serious medical condition (Stein et al., 2019). It is a cycle where the brain’s “alarm system” goes off by mistake, creating a sense of immediate danger even when everything is fine. This cycle is driven by obsessions, which are unwanted thoughts or images that pop into your head and cause a lot of stress (American Psychiatric Association [APA], 2022).
To stop the bad feeling, people perform compulsions. These can be physical actions (like washing) or mental compulsions—such as mental checking, rumination, or praying—that are often invisible to others (Mancebo et al., 2005). While these rituals make you feel better for a second, they actually trick the brain into thinking the danger was real, which keeps the cycle going (Abramowitz & Jacoby, 2015).
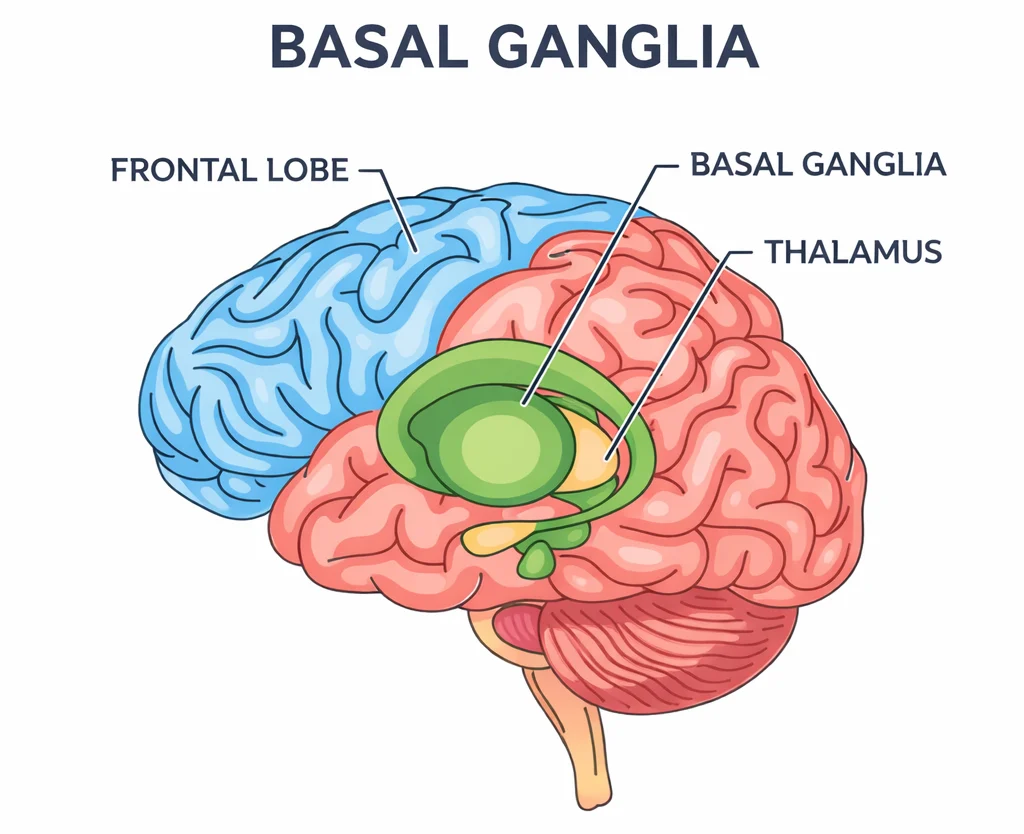
Understanding the "Brain Brake" (The Basal Ganglia)
To understand why this happens, it helps to look at a part of the brain called the basal ganglia. You can think of this area as the “Brain Brake.” In a typical brain, when you have a random thought like “Did I lock the door?”, the basal ganglia helps you check once and then “brakes” the thought so you can move on. In an OCD brain, that brake is slippery or broken (Knowles et al., 2020; Robbins et al., 2019). The thought keeps spinning and spinning because the brain can’t find the “stop” button.
The Spectrum of Obsessions: Mental and Physical
The themes of OCD are different for everyone and often attack the things a person cares about most. Because these thoughts are ego-dystonic, they represent the exact opposite of who the person really is (Wheaton et al., 2021). It is vital to know that these are just symptoms of a medical disorder and do not mean the person actually wants to do these things. Because symptoms can be subtle, specialized screening in clinics is often necessary to catch them early (Zimmerman et al., 2013).
- Harm OCD: Fear of hurting others or yourself accidentally or on purpose (Veale et al., 2014).
- Mental Contamination: Feeling “dirty” because of a bad thought or a mean person, even without physical contact (Rachman, 2006).
- Symmetry and Order: A powerful need for things to be “just right” to prevent a vague disaster (Radomsky et al., 2010).
- Taboo Thoughts: Intrusive sexual or religious images that feel “wrong” to the sufferer (Mancebo et al., 2005). This includes Sexual Orientation OCD (SO-OCD), where a person fears their sexual identity has changed against their will (Williams et al., 2014).
- Responsibility OCD: Feeling personally responsible for preventing every possible bad thing (Salkovskis, 1985).
Important Distinction: Do not confuse OCD with Obsessive-Compulsive Personality Disorder (OCPD). OCD involves thoughts the person hates (ego-dystonic), while OCPD involves a person who believes their perfectionism is the “right” way for everyone to act (ego-syntonic) (Fineberg et al., 2007).
Distinguishing Intrusive Thoughts: OCD vs. PTSD
Comparison Table: Understanding the Difference
Feature
OCD
PTSD
Origin
“What-if” fears about the future.
Flashbacks of real past events.
Focus
Doubting your character or safety.
Re-living a specific trauma.
Goal
Trying to prevent a hypothetical disaster.
Trying to stay safe from a past threat.
One major rule that providers follow is that OCD causes anxiety, but anxiety does not cause OCD (Farris et al., 2019). Because the “glitch” in OCD is neurobiological, you cannot simply worry your way into the disorder. For those who struggle with both, providers often suggest working on the trauma memories first. Once the nervous system feels safer, it becomes much easier for the individual to distinguish between a “trauma memory” and an “OCD loop” (Wheaton et al., 2021).
PANS and PANDAS: Sudden Medical Emergencies
Usually, OCD starts slowly (Geller et al., 2017), but for some kids, it shows up “overnight.” This is called Pediatric Acute-Onset Neuropsychiatric Syndrome / Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANS/PANDAS).
It happens when an infection (like Strep throat) causes the body’s immune system to get confused. Instead of just fighting germs, the antibodies attack the “Brain Brake” (basal ganglia), causing the brain to become swollen (Murphy et al., 2015; Swedo et al., 2015; Wilcox et al., 2014).
Red Flags for PANS/PANDAS:
- Sudden Onset: OCD symptoms appear literally in 24-48 hours (Lewin et al., 2018).
- Restricted Eating: The child suddenly fears food is “poisoned” or they will choke.
- Age Regression: A 10-year-old suddenly acts like a 4-year-old (baby talk, bedwetting).
- Physical Tics: Sudden jerky movements or repetitive sounds (Postorino et al., 2017).
URGENT MEDICAL DISCLAIMER: We are educational providers, not medical prescribers. If your child suddenly develops severe OCD or restricted eating after being sick, call your Primary Care Provider (PCP) immediately. Early medical treatment like antibiotics is critical to stop the brain swelling (Cunningham et al., 2021).
Family Dynamics: Supportive Non-Accommodation
OCD is often called a “family disorder” because it affects everyone in the house. Because they love the person, family members often “help” by providing reassurance or doing rituals—this is called Family Accommodation. While this makes things calm for a few minutes, research shows that it actually makes the OCD stronger over time (Calvocoressi et al., 2016).
The best way for a family to help is supportive non-accommodation. This involves identifying common traps like reassurance-seeking. When a family member answers the question “Are you sure the stove is off?”, they are accidentally completing a compulsion for the sufferer. Instead, family members should say:
“I can see you are really scared right now, and I’m so sorry you’re hurting. But because I love you and want you to get better, I am not going to answer that ‘what-if’ question for you.”
When the family stops “feeding” the OCD rituals, the person with OCD learns that they can handle the scary feeling on their own (Lebowitz et al., 2020).
The Path to Recovery: ERP vs. Traditional Therapy
The best treatment for OCD is Exposure and Response Prevention (ERP). It is vital to distinguish ERP from traditional “talk therapy.” While talk therapy often looks for “root causes” or “hidden meanings”—which can actually act as a form of rumination and make OCD worse—ERP focuses solely on the response to the thought (Abramowitz & Jacoby, 2015).
ERP asks you to face your fears without doing a ritual. This helps your brain learn habituation, which means your brain “gets bored” of being scared (Hezel & Simpson, 2019). This cycle can even be effectively addressed through remote therapy options (Wootton, 2016).
In a session, you might use a script while facing a fear:
“I am having the thought that I could be dangerous. I don’t know for 100% sure that I’m safe, and I am going to sit here with that feeling until my brain realizes I am okay.”
By staying with the fear and refusing to do the ritual, your brain eventually realizes the alarm was a mistake. This is how you find real, long-term relief (Hofmann et al., 2017).
Conclusion: Hope and Relapse Prevention
Living with OCD can feel like being a prisoner, but relief is possible even in cases that seem “treatment-resistant” (Shavitt et al., 2019). It is important to remember that recovery doesn’t mean you will never have a weird thought again. Instead, it means you have a “toolbox” of skills like ERP to handle those thoughts so they don’t turn into a cycle.
Even if you have a “setback,” you are not back at square one. You now know how the “Brain Brake” works and how to use ERP to stay in control. Relief comes from learning that you don’t need a “perfect” answer to your questions to be safe and happy. You are not alone, and there is a bright life waiting for you once you stop the cycle of compulsions.
Resources
Abramowitz, J. S., & Jacoby, R. J. (2015). The use of exposure and response prevention for OCD. The Bulletin of the Menninger Clinic, 79(2), 116–144.
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.).
Calvocoressi, L., et al. (2016). Family accommodation in OCD. Journal of Obsessive-Compulsive and Related Disorders, 9, 48–56.
Cunningham, N. R., et al. (2021). Relationship between PANS/PANDAS and OCD symptoms. Journal of Child and Adolescent Psychopharmacology, 31(3), 150–158.
Farris, S. G., et al. (2019). The role of anxiety sensitivity in OCD. Cognitive Behaviour Therapy, 48(4), 312–325.
Fineberg, N. A., et al. (2007). Obsessive-compulsive personality disorder: A review. The British Journal of Psychiatry, 191(3), 204–210.
Geller, D. A., et al. (2017). Clinical features of pediatric-onset OCD. Psychiatric Clinics, 40(3), 401–415.
Hezel, D. M., & Simpson, H. B. (2019). Exposure and response prevention for OCD. Focus, 17(1), 14–20.
Hofmann, S. G., et al. (2017). The efficacy of cognitive behavioral therapy: A review of meta-analyses. Cognitive Therapy and Research, 36(5), 427–440.
Knowles, E. E., et al. (2020). The genome-wide anatomy of OCD. Nature Communications, 11(1), 1–10.
Lebowitz, E. R., et al. (2020). Family accommodation in pediatric OCD. Child and Adolescent Psychiatric Clinics, 29(3), 545–556.
Lewin, A. B., et al. (2018). PANS/PANDAS: Clinical management and research. Journal of Child and Adolescent Psychopharmacology, 28(1), 2–15.
Mancebo, M. C., et al. (2005). Taboo obsessions in OCD. Journal of Nervous and Mental Disease, 193(10), 687–693.
Murphy, T. K., et al. (2015). Clinical factors in PANDAS. Journal of Child and Adolescent Psychopharmacology, 25(1), 19–30.
Pittenger, C. (2017). Obsessive-compulsive disorder: Phenomenology, pathophysiology, and treatment. Oxford University Press.
Postorino, V., et al. (2017). Clinical characteristics of children with PANDAS. Journal of Child and Adolescent Psychopharmacology, 27(8), 715–722.
Rachman, S. (2006). The Fear of Contamination. Oxford University Press.
Radomsky, A. S., et al. (2010). Cognitive behavioral treatment for symmetry-related OCD. Journal of Cognitive Psychotherapy, 24(3), 184–196.
Robbins, T. W., et al. (2019). Obsessive-compulsive disorder: Puzzles and prospects. Neuron, 102(1), 27–47.
Salkovskis, P. M. (1985). Obsessional-compulsive problems: A cognitive-behavioural analysis. Behaviour Research and Therapy, 23(5), 571–583.
Shavitt, R. G., et al. (2019). Treatment-resistant OCD. Focus, 17(1), 21–29.
Stein, D. J., et al. (2019). Obsessive-compulsive disorder. Nature Reviews Disease Primers, 5(1), 1–21.
Swedo, S. E., et al. (2015). Clinical definition of PANS. Journal of Child and Adolescent Psychopharmacology, 25(1), 3–17.
Van Ameringen, M., et al. (2014). The overlap between OCD and PTSD. Journal of Clinical Psychiatry, 75(0), 1–10.
Veale, D., et al. (2014). Treatment of harm obsessions in OCD. The Psychiatrist, 38(2), 73–77.
Wheaton, M. G., et al. (2021). Intrusive thoughts in OCD vs. PTSD. Journal of Anxiety Disorders, 78, 102356.
Wilcox, J. A., et al. (2014). PANS and PANDAS: An overview. Clinical Pediatrics, 53(9), 830–835.
Williams, M. T., et al. (2014). Sexual orientation OCD. The Journal of Obsessive-Compulsive and Related Disorders, 3(3), 284–291.
Wootton, B. M. (2016). Remote cognitive-behavioral therapy for OCD. Clinical Psychology: Science and Practice, 23(1), 22–31.
Zimmerman, M., et al. (2013). Screening for OCD in an outpatient clinic. Journal of Clinical Psychiatry, 74(4), 382–386.