
OCD Explained: Symptoms, Intrusive Thoughts, and ERP Treatment

Understanding Scrupulosity:
When OCD Masks Itself as Faith
Erik Turley, LMFT
07/13/2026
For many people, faith is a source of peace, comfort, and community. But for those living with an underrecognized type of Obsessive-Compulsive Disorder (OCD), religious devotion can slowly turn into a source of constant fear, guilt, and exhaustion. This specific presentation of OCD is known as scrupulosity.
If you or a loved one are struggling to separate sincere faith from a mental health condition, you are not alone. Let’s break down what scrupulosity is, how it feeds on highly valued religious principles, and what scientific research tells us about finding relief.
What Exactly is Scrupulosity?
In standard OCD, a person experiences obsessions—unwanted, intrusive thoughts or urges that cause heavy anxiety—and performs compulsions, which are repetitive behaviors or mental acts aimed at making that anxiety go away.
When a person has scrupulosity, their obsessions and compulsions target their moral or religious beliefs (Buchholz et al., 2019). It acts like a glitch in the brain’s alarm system, making a person feel like they are constantly sinning, displeasing God, or violating a sacred rule, even when they are doing their absolute best.
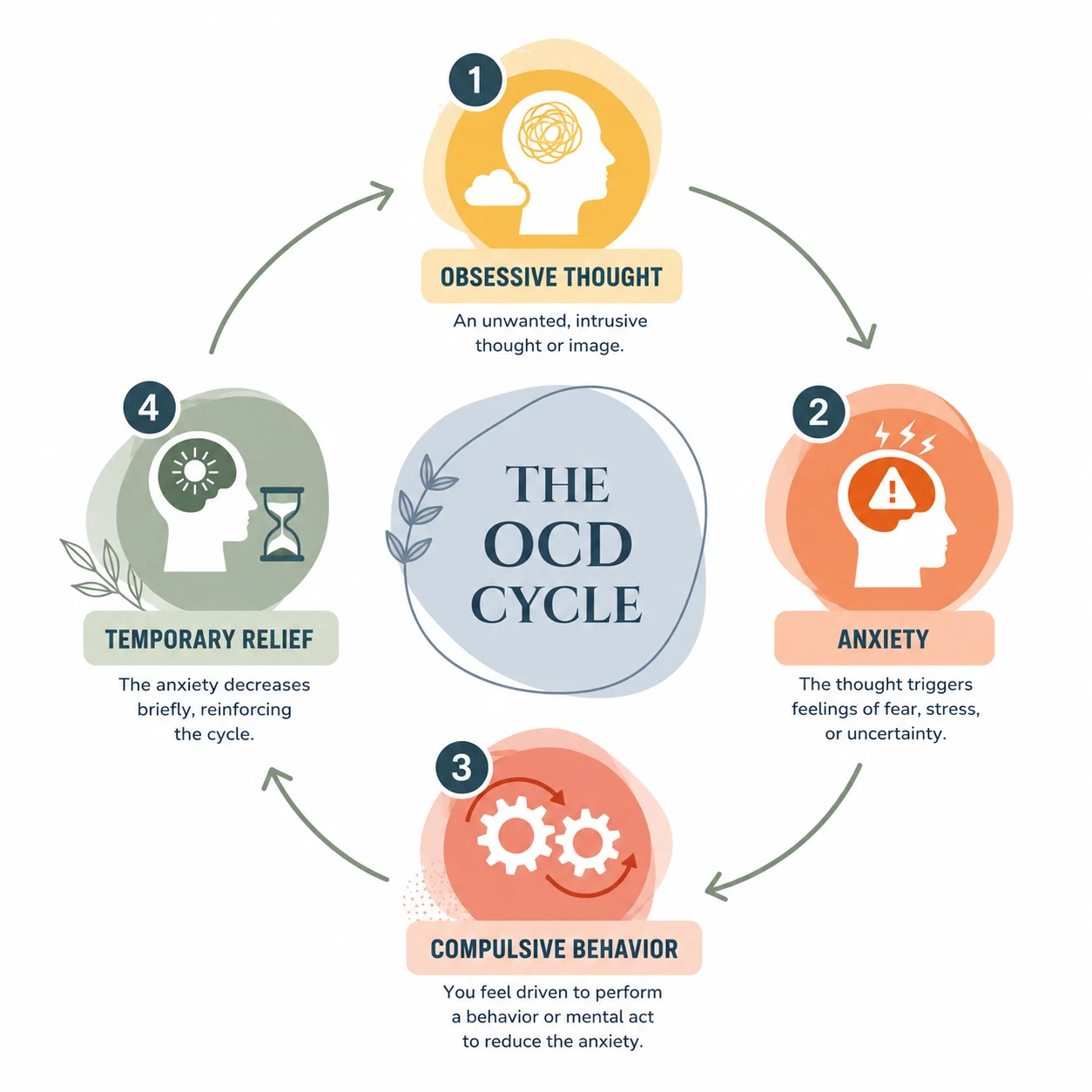
As shown in the cycle above, scrupulosity traps an individual in a repeating loop:
- Obsessive Thought: An intrusive doubt arises (e.g., “Did I say that prayer with enough sincerity?” or “Was that random thought a sin?”).
- Anxiety: The brain sounds an emergency alarm, triggering deep fear of divine punishment or moral failure.
- Compulsive Behavior: The person tries to fix the feeling by praying repeatedly, over-confessing, or asking religious leaders for reassurance.
- Temporary Relief: The anxiety dips for a moment, but the brain quickly learns that the compulsion “saved” them, reinforcing the vicious loop next time a doubt pops up.
The Perfectionism Trap: Outperforming the Deity
The core engine of scrupulosity is a heavy dose of maladaptive perfectionism—setting impossibly high standards and viewing anything less than absolute flawlessness as a total moral failure (Dyer et al., 2023).
Individuals struggling with this condition often unknowingly rewrite the rules of their own faith. They end up holding themselves to a significantly higher, more rigid standard than their actual religious doctrines, scriptures, or deity require.
Standard Religious Practice
Repentance & Grace: Mistakes happen; a person sincerely corrects them and relies on divine mercy.
Human Limitations: Faith doctrines generally accept that humans have intrusive thoughts or complex feelings.
Faith & Trust: Living with the understanding that humans cannot know everything, but trusting in divine goodness.
Scrupulosity / Perfectionism
Flawless Execution: Mistakes are unacceptable. If a prayer or confession isn’t 100% “perfectly felt,” it doesn’t count.
Thought-Action Fusion: Believing that a random, unwanted thought is just as sinful as physically committing an evil act.
Intolerance of Uncertainty: An absolute demand for concrete proof that one is totally forgiven and “safe.”
The Intolerance of Anxiety and Fear
While a demand for absolute perfection drives the thoughts, an intolerance of anxiety drives the frantic behaviors. Sufferers do not just fear God or sin; they grow to deeply fear the feeling of anxiety itself.
Research shows that people with scrupulosity struggle heavily with distress intolerance—the perceived inability to survive or cope with uncomfortable emotions (Reuman et al., 2017). When a wave of religious doubt hits, the accompanying spike of fear feels completely unlivable. Sufferers mistakenly view their internal anxiety as a spiritual warning system, concluding: “If I am feeling this much panic and guilt, it must mean I am actually guilty and God is angry at me.”
Furthermore, they may develop a belief that experiencing anxiety or fear is inherently sinful. They think that if their faith were strong enough, they would feel perfect peace. This creates a painful meta-anxiety (anxiety about having anxiety), forcing them to perform compulsions not just to fix a spiritual problem, but to desperately escape the emotional discomfort.
The Intersection of Faith and OCD
A common point of confusion is the difference between normal religiosity (devotion to and practice of one’s religion) and clinical scrupulosity. Research consistently shows that scrupulosity is not caused by having strong religious beliefs (Bailey et al., 2023). Instead, OCD simply latches onto what matters most to a person. If you care deeply about your faith, OCD will use your faith to frighten you.
Different faith traditions see scrupulosity express itself in unique ways based on their specific doctrines:
- The Church of Jesus Christ of Latter-day Saints (LDS or Mormon): In Latter-day Saint culture, doctrines emphasizing eternal progression, personal worthiness, and commandments can sometimes be misinterpreted by a perfectionistic, anxious brain. Research highlights that an intolerance of uncertainty plays a huge role here (Christensen, 2019). An LDS individual with scrupulosity might obsess over whether they repented perfectly, or they might confess minor, normal human mistakes to their bishop over and over out of a toxic need for absolute certainty.
- Protestantism and Catholicism: Christian doctrines regarding the “Sermon on the Mount”—where thoughts are held to high moral standards—can trigger severe scrupulosity. Sufferers often experience thought-action fusion (Buchholz et al., 2019). They may spend hours analyzing their minds for any “blasphemous” or impure thoughts, creating a standard of mental purity that is functionally impossible to hit.
- Islam and Judaism: In these traditions, scrupulosity frequently zeroes in on ritual purity and exactness. Sufferers may experience intense checking rituals, such as repeating ritual washings (wudu in Islam) or obsessively worrying if their food strictly met kosher or halal rules, fearing the entire practice was ruined by a tiny, accidental error.
The Breaking Point: Walking Away From Faith
One of the most heartbreaking outcomes of severe scrupulosity happens when the constant, agonizing anxiety becomes completely unlivable. Out of pure emotional exhaustion, some individuals choose to walk away from their faith, drop their religious practices, and abandon their deeply held morals or values.
To an outsider—or to the sufferers themselves—it looks like a loss of faith. In reality, it is a massive avoidance compulsion. The person’s brain tells them: “If I just step away from religion altogether, the rules will disappear, and the terrifying anxiety will finally stop.” Unfortunately, because OCD is a structural glitch in how the brain processes doubt—not a reflection of actual religious doctrine—leaving the faith rarely stops the cycle. Instead, individuals experience a phenomenon known as symptom migration, where the target of a person’s OCD changes, but the underlying anxiety cycle stays exactly the same (Brakoulias et al., 2017). The underlying anxiety and perfectionism stay exactly where they are, but they quickly find a new, secular target that the person still cares about:
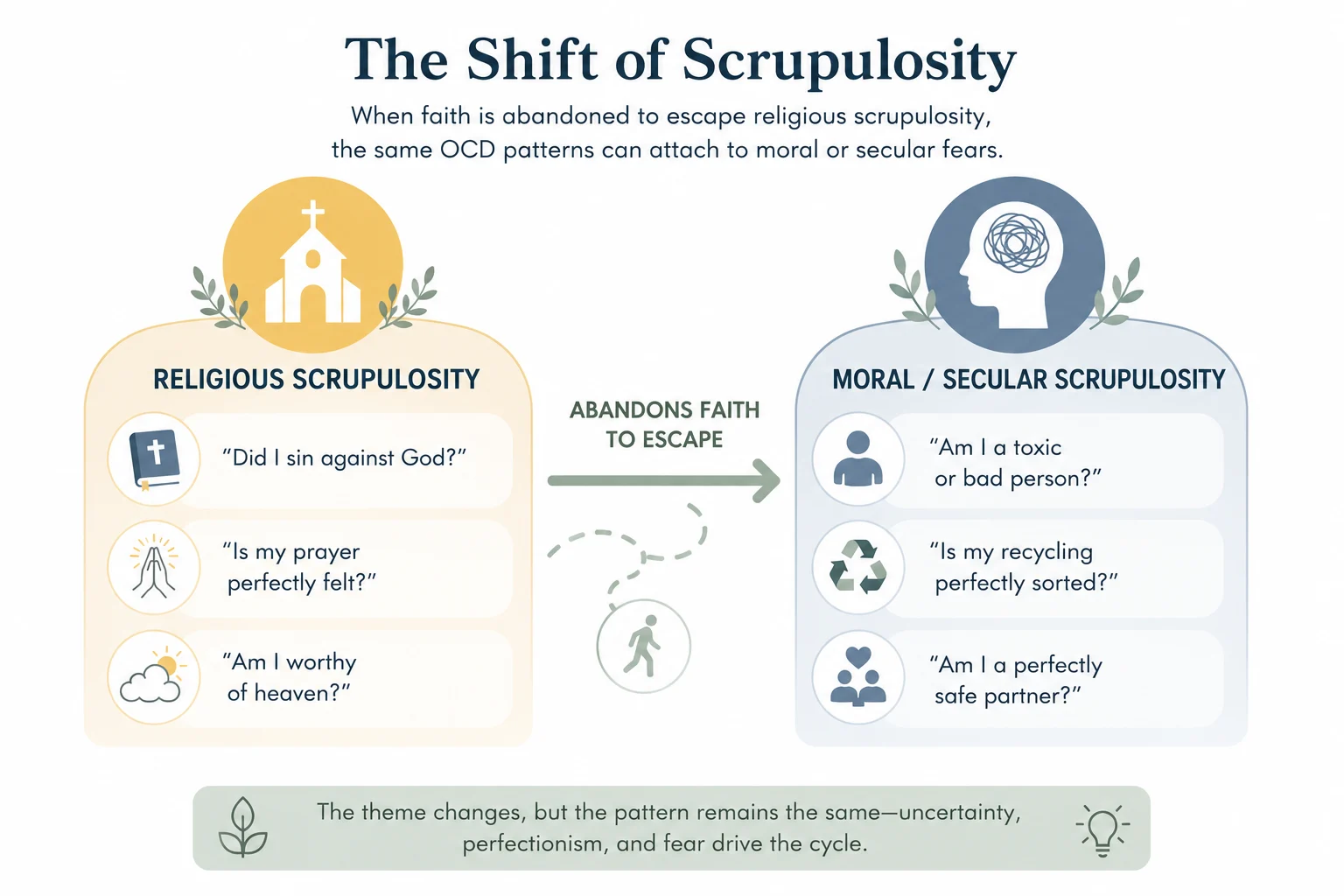
Once the faith is dropped, the perfectionistic energy typically transforms into:
- Moral Scrupulosity: The obsession shifts from pleasing a deity to being a “perfectly good secular person.” Sufferers obsess over whether they are accidentally causing harm to others, being selfish, or acting unethically (Purdon & Clark, 2005).
- Relationship OCD (ROCD): The absolute demand for certainty moves into human relationships. The brain relentlessly attacks their love life with unanswerable questions: “Do I actually love my partner? Do they love me? Did I look at that stranger too long, and does that mean I’m a liar?”
- Hyper-Environmentalism or Social Justice: The need for flawless compliance latches onto worldly ethics. A person might face paralyzing guilt over whether they threw away a piece of plastic incorrectly or consumed a product that wasn’t ethically sourced.
Walking away from values out of sheer exhaustion is a tragic survival mechanism. It highlights a critical truth: the problem was never the religion itself; it was the untreated OCD.
What Does the Science Say?
Mental health professionals utilize specific scientific data to understand and treat this condition:
It is a Bridge Condition: A study utilizing network analysis—a research method that maps out how different symptoms connect to one another—found that scrupulosity serves as a literal bridge between everyday spiritual struggles and clinical OCD symptoms (Moroń et al., 2022). This means addressing it requires care from both a psychological perspective and a supportive religious viewpoint.
Perfectionism is a Catalyst: Studies indicate that perfectionism directly fuels depression and anxiety within religious communities, including among Latter-day Saints (Dyer et al., 2023).
A Brain Processing Deficit: Neuroscientific research shows that individuals with high obsessive-compulsive traits struggle with Bayesian inference—a mathematical way the brain is supposed to use past experiences to accurately predict the present or future (Stern et al., 2020). Because their brains cannot rely on past data (like a past confession or a logical realization that they are a good person), they experience severe, ongoing doubt and overreact to tiny errors.
High-Level Psychological Terms Defined
To help understand scientific texts on this topic, here are key terms defined simply:
- Ego-dystonic: Thoughts, impulses, or behaviors that completely contradict a person’s true beliefs, self-image, and core values. (e.g., A deeply loving religious person experiencing horrifying thoughts of committing blasphemy).
- Cognitive Restructuring: A core therapy method used to identify, challenge, and alter unhelpful, inaccurate, or negative thought patterns.
- Distress Intolerance: The mental setting where a person finds normal emotional pain or anxiety completely unbearable, leading them to do anything to escape the feeling immediately.
- Maladaptive: Behaviors or thought processes that prevent a person from adapting cleanly or healthily to situations, often making anxiety worse rather than solving it.
- Symptom Migration: The clinical reality where a patient’s old physical or mental compulsions improve, but the underlying OCD redirects its focus toward a brand-new theme (Wheaton et al., 2021).
- Thought-Action Fusion: The psychological error of treating an internal thought as identical to a real-world physical action.
Moving Forward
The gold standard treatment for scrupulosity is Exposure and Response Prevention (ERP), a form of cognitive behavioral therapy where individuals gradually face their anxious doubts without performing the comforting rituals or compulsions. Clinical trials show that ERP modified specifically for scrupulosity significantly drops a person’s distress levels and allows them to successfully return to a flexible spiritual life (Abramowitz et al., 2014; Huppert & Siev, 2010).
Through ERP, individuals learn an essential truth: they can feel intense anxiety and uncertainty, and nothing terrible will happen if they sit with it. Over time, as they practice tolerating the emotional discomfort without fighting it, the brain’s false alarm system naturally quietens down. When paired with a religious leader who understands OCD, individuals can learn to tolerate the uncertainty of life while maintaining a healthy, loving, and balanced relationship with their faith.
Resources and Academic References
- International OCD Foundation (IOCDF) Faith Guides: IOCDF Faith and OCD Resources
- Support Groups: The National Alliance on Mental Illness (NAMI) and local OCD support groups.
References
Abramowitz, J. S., Jacoby, R. J., & Jordan, K. D. (2014). Exposure and response prevention for scrupulosity: Technical modifications and clinical challenges. Cognitive and Behavioral Practice, 21(3), 307–317. https://doi.org/10.1016/j.cbpra.2013.12.002
Bailey, C., Venta, A., Baumgartner, M., Mercado, A., Colunga-Rodríguez, C., Ángel-González, M., Dávalos-Picazo, G., & Sarabia-López, L. E. (2023). Religiosity and religious scrupulosity as markers of poor mental health in the Latinx community: A mediation model. Practice Innovations, 8(1), 23–33. https://doi.org/10.1037/pri0000208
Brakoulias, V., Starcevic, V., Albert, U., Arumugham, S. S., Bailey, B. E., Belloch, A., … & Fineberg, N. A. (2017). Treatments utilized for obsessive-compulsive disorder (OCD) and the stability of its symptom dimensions: A prospective international study. International Journal of Psychiatry in Clinical Practice, 21(3), 195–201. https://doi.org/10.1080/13651501.2017.1306079
Buchholz, J. L., Abramowitz, J. S., Riemann, B. C., Reuman, L., Blakey, S. M., Leonard, R. C., & Thompson, K. A. (2019). Scrupulosity, religious affiliation and symptom presentation in Obsessive Compulsive Disorder. Behavioural and Cognitive Psychotherapy, 47(4), 478–492. https://doi.org/10.1017/S1352465818000711
Christensen, M. R. (2019). Scrupulosity and Latter-day Saints: The potential benefits of tolerating uncertainty. Intuition: The BYU Undergraduate Journal of Psychology, 14(1), Article 3. https://scholarsarchive.byu.edu/intuition/vol14/iss1/3/
Dyer, W. J., Judd, D. K., Gale, M., & Finlinson, H. G. (2023). Religion, mental health, and the Latter-Day Saints: A review of literature 2005–2022. Religions, 14(6), 701. https://doi.org/10.3390/rel14060701
Huppert, J. D., & Siev, J. (2010). Treating scrupulosity in religious individuals using cognitive-behavioral therapy. Cognitive and Behavioral Practice, 17(4), 382–392. https://doi.org/10.1016/j.cbpra.2009.07.003
Moroń, M., Biolik-Moroń, M., & Matuszewski, K. (2022). Scrupulosity in the network of obsessive-compulsive symptoms, religious struggles, and self-compassion: A study in a non-clinical sample. Religions, 13(10), 879. https://doi.org/10.3390/rel13100879
Purdon, C., & Clark, D. A. (2005). Overcoming obsessive thoughts: How to gain control of your OCD. New Harbinger Publications.
Reuman, L., Jacoby, R. J., Fabricant, L. E., Brand, J., & Abramowitz, J. S. (2017). Uncertainty as an enemy: The role of distress intolerance and intolerance of uncertainty in scrupulosity. Journal of Obsessive-Compulsive and Related Disorders, 12, 43–48. https://doi.org/10.1016/j.jocrd.2016.12.001
Skoog, G., & Skoog, I. (1999). A 40-year follow-up of patients with obsessive-compulsive disorder. Archives of General Psychiatry, 56(2), 121–127. https://doi.org/10.1001/archpsyc.56.2.121
Stern, Y., Avila, J. F., & Shaked, D. (2020). Doubting what you already know: Uncertainty regarding state transitions is associated with obsessive compulsive symptoms. PLOS Computational Biology, 16(3), e1007468. https://doi.org/10.1371/journal.pcbi.1007468
Wheaton, M. G., Ward, H. E., & Silber, A. (2021). Changing faces of OCD: Managing symptom substitution and migration across the lifespan. Journal of Obsessive-Compulsive and Related Disorders, 29, 100632. https://doi.org/10.1016/j.jocrd.2021.100632